2022-2023 Influenza Season: Activity and Vaccine Effectiveness - Pharmacy Times
Influenza is a viral disease that spreads from person to person and typically circulates from October to May in the Northern Hemisphere.1,2 Mild to moderate illness is common. Approximately 8.8% of adults younger than 65 years of age experience influenza infection (flu). Children are most likely (9.3%) to contract the flu, whereas older adults (those 65 years and older) are less likely (4.9%). However, among older adults and those with chronic diseases who do develop an influenza infection, severe disease and death are more likely.1 The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), or COVID-19, was recognized in late 2019; the subsequent pandemic caused by this virus has influenced global influenza activity.3 The CDC speculated that mitigation measures that were put in place to combat COVID-19 also led to a global decline in the number of influenza cases in the 2020-2021 season.4 In the 2021-2022 season, influenza cases were higher than the year before, but lower than pre-pandemic levels. There was bimodal activity, which peaked in late December 2021 and April 2022. The season extended into June, making it the longest spring activity on record.5
Axel Kock - stock.adobe.com
Influenza Activity for the 2022-2023 Season
During the 2022-2023 influenza season, 10% of total respiratory samples were positive for influenza; these were dominated by influenza A (97.8%), primarily H3N2 (72.4%).6 In the 2021-2022 season, influenza activity had a bimodal pattern, with a positivity slightly above 6% in December 2021; this decreased to approximately 2% in January 2022, and peaked again in April 2022 with 10% positivity.5,7 Health care visits for influenz-alike illnesses peaked at 7.5% at the end of November 2022, staying above the baseline threshold of 2.5% for 21 weeks, and did not demonstrate a bimodal pattern of activity.8
The National Center for Health Statistics now reports mortality surveillance for pneumonia, influenza, and COVID-19. Compared with influenza, most deaths for the current season are attributable to COVID-19. Mortality and hospitalization for influenza were similar to those of pre-pandemic years. Notably, hospitalizations peaked earlier in the season than in any of the past 8 seasons.6 There were 158 pediatric deaths in the 2022-2023 season compared with 47 in the previous 2 seasons combined. These totals are less than the 199 pediatric deaths observed in the largely pre-pandemic 2019-2020 season.
Influenza Virus Classification
There are 2 main lineages of human influenza viruses, type A and type B.9 For type A, viruses are subdivided by their major antigenic markers—hemagglutinin and neuraminidase. This season, 98% of cases are attributable to type A influenza. The H3N2 strain, which has been circulating since its introduction in the United States during the 1968 pandemic, accounts for 72.4% of type A cases; (H1N1)pdm09, the strain from the 2009 pandemic, accounts for 27.6% of type A cases.6,10
Influenza Vaccines
Factors that determine influenza vaccine composition each year include epidemiologic data (ie, which influenza viruses are circulating around the world at different locations and times) and genetic and antigenic changes.11 The year-to-year genetic mutations that allow influenza to partially evade our antibodies is called antigenic drift.12 This differs from antigenic shift, where there is a major change in the hemagglutinin or neuraminidase proteins and the population may have no immunity to the new virus, resulting in a pandemic. No clinically significant resistance to neuraminidase inhibitors has been observed with the circulating strains this season.6
Available Vaccine Products
Nine influenza vaccines—1 live-attenuated and 8 inactivated—were available during the 2022-2023 influenza season (Table).2 The FDA licenses influenza vaccines for individuals 6 months of age and older; this aligns with the recommendations from the CDC's Advisory Committee on Immunization Practices (ACIP).
Table From Pharmacy Times 2023 Influenza Guide for Pharmacists
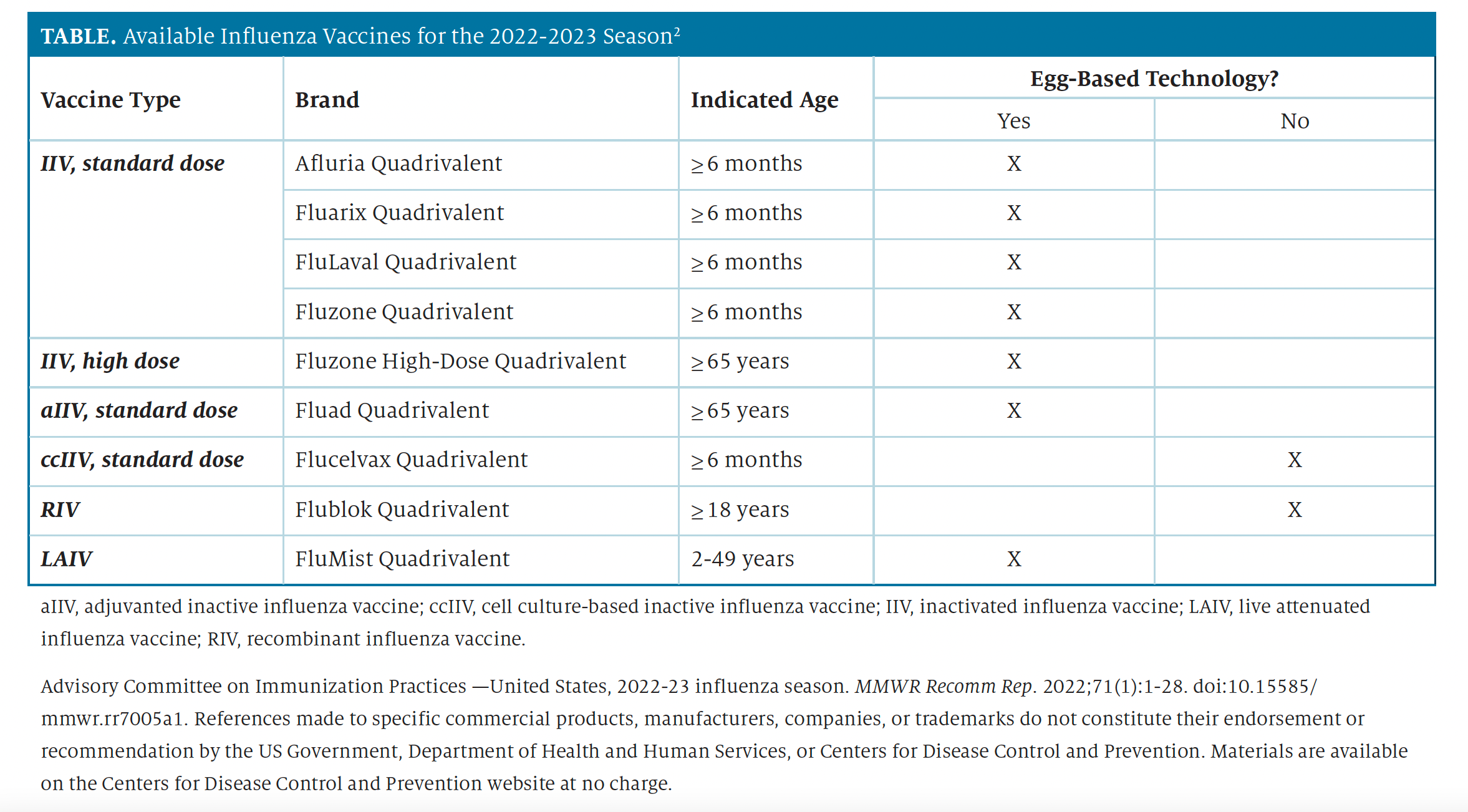
All influenza vaccines currently marketed in the United States are quadrivalent, meaning that they target 1 type A(H3N2) virus, 1 type A(H1N1) virus, 1 type B virus of the Yamagata lineage, and 1 type B virus of the Victoria lineage.2,9 All influenza vaccines in the United States contain the same major type A and B strains, but they may differ slightly based on the technology used to manufacture them.2 Egg-based vaccines have been around for more than 70 years13; however, newer methods to avoid egg adaptation involve cell culture or recombinant technology to create influenza vaccines (Table).2,13,14 The advantage of using these newer methods to create influenza vaccines is that they may offer a higher degree of protection compared with traditional egg-based products and can be administered to individuals with egg allergies.2,14,15 The 2 non-egg–based vaccines available are Flucelvax Quadrivalent, which is a cell-culture–based inactivated influenza vaccine, and Flublok Quadrivalent, which is a recombinant influenza vaccine.2
ACIP Recommendations
Key changes to the ACIP recommendations for influenza vaccines in the 2022-2023 season included2:
- Afluria Quadrivalent likely will not be available in 0.25-mL prefilled syringes. For children 6 months to 35 months of age who need this dose, Afluria Quadrivalent must be obtained from a multidose vial.
- Flucelvax Quadrivalent is now approved for individuals aged 6 months or older.
- Adults aged 65 years or older should preferentially receive 1 of the following higher dose or adjuvant vaccines: quadrivalent high-dose inactivated influenza vaccine, quadrivalent recombinant influenza vaccine, or quadrivalent adjuvant inactivated influenza vaccine. However, if none of these vaccines are available, then any other ageappropriate influenza vaccine should be used.
In March 2023, the FDA voted to approve the 2023-2024 seasonal influenza vaccine composition.16 All influenza vaccines available in the United States will remain quadrivalent, offering protection against the most common types of A and B influenza viruses.11 Although there was no change from the 2022-2023 season for the H3N2, B/Yamagata, and B/Victoria components, the H1N1 strain was changed for the upcoming 2023 to 2024 season.16
The following strains are to be used by manufacturers for the 2023-2024 season16:
- A/H1N1 — A/Victoria/4897/2022 pdm09-like virus (for egg-based vaccines) or an A/Wisconsin/67/2022 pdm09-like virus (for cellor recombinant-based vaccines);
- A/H3N2 — an A/Darwin/9/2021-like virus (for egg-based vaccines) or an A/Darwin/6/2021-like virus (for cell- or recombinant-based vaccines);
- B — B/Phuket/3073/2013-like virus (B/Yamagata lineage);
- B — B/Austria/1359417/2021-like virus (B/Victoria lineage).
Administration
The influenza vaccine is administered intramuscularly or intranasally (ie, the live attenuated influenza vaccine) with appropriate dose and age range determined by the specific product formulation and FDA indication.17 Unless there is a contraindication to receiving the influenza vaccine, everyone aged 6 months or older should be vaccinated annually by the end of October. Immunization efforts should start in September or October in advance of the influenza season, which historically peaks in February. Children who need 2 doses can receive the vaccine as soon as it is available (generally around July or August); however, adults, particularly those aged 65 years or older and women who are pregnant and in their first or second trimester, should not receive it early due to concerns of a waning immune response during the remainder of the influenza season.2
Effectiveness of the 2022-2023 Seasonal Influenza Vaccines
The effectiveness of influenza vaccines varies each season and is determined by the circulating influenza virus subtype(s) and the extent to which there is an antigenic match in the vaccines to the circulating virus subtypes.18 For the 2021-2022 season, vaccine effectiveness (VE) for the predominant influenza A(H3N2) virus was 36% overall, with the highest effectiveness seen in individuals 6 months to 8 years of age (43%) and the lowest effectiveness observed in individuals aged 50 years or older (10%).19
For the 2022-2023 season, influenza activity began earlier than expected in the United States and increased in October 2022.18 There were high rates of influenza-associated hospitalizations among children. Most cases of influenza were attributed to A/H3N2, but A/H1N1pdm09 circulated as well. An interim estimate of VE for influenza A for the 2022-2023 season was 54% in individuals aged 6 months to 64 years. Patients aged 65 years or older were excluded from this interim VE estimate. These preliminary results suggest a similar if not slightly better vaccine match to circulating strains than in previous pre-pandemic years.20 According to the CDC, from 2017 to 2022, VE for influenza vaccines has ranged from 29% to 40%. Since influenza VE is generally less in individuals aged 65 years or older, high-dose (Fluzone High Dose), recombinant (Flublok), and adjuvant (Fluad) vaccines are now preferentially recommended by the CDC for the prevention of influenza, hospitalization, and death in this population.2
More Work to be Done — Role of Pharamcists in Increasing Influenza Vaccine Uptake
During the 2022-2023 influenza season, the CDC reported that pharmacies administered 41.48 million doses of influenza vaccines to adults aged 18 years and older, an increase of 1.02 million doses from the previous year.21 This surpassed the number of doses administered in physicians' medical offices (27.96 million, which was 2.93 million fewer doses compared with the previous year). The 2022-2023 influenza vaccination rate in adults aged 65 years and older rose 3.7% from the previous influenza season to 71.0%; this population represented the largest group of adults vaccinated this influenza season.22 Despite the increased vaccine uptake, the CDC estimates that 3 of every 4 adults are missing 1 or more routinely recommended vaccines, including influenza.23
However, influenza vaccination rates among children were similar during the past 2 seasons; 55.6% were vaccinated during the 2022-2023 season compared with 55.1% during the 2021-2022 season.24 These comparable influenza vaccination rates may represent a lingering effect of the COVID-19 pandemic, when rates of pediatric immunizations declined. The CDC produced a guide with talking points for pharmacists to help increase influenza vaccination uptake.25 It addresses vaccine hesitancy in patients and aims to improve vaccine confidence. Although influenza rates decreased during the early phases of the COVID-19 pandemic, they have returned to pre-pandemic levels. Each season it will take the efforts of pharmacists and other health care providers to get everyone vaccinated for influenza and, likely, COVID-19.
About the Author
Jeff Goad, PharmD, MPh, APh, is a professor and associate dean of
academic affairs at the Chapman University School of Pharmacy in Irvine,
California.
Karl Hess, PharmD, APh, is an associate professor and director of
experiential education at the Chapman University School of Pharmacy in
Irvine, California.
References
- Key facts about influenza (flu). CDC. October 24, 2022. Accessed June 19, 2023. https://www.cdc.gov/flu/about/keyfacts.htm
- Grohskopf LA, Blanton LH, Ferdinands JM, et al. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices, United States, 2022-23 Influenza Season. MMWR Recomm Rep. 2022;71(1):1-28. doi:10.15585/mmwr.rr7005a1
- Coronavirus disease (COVID-19). World Health Organization. March 28, 2023. Accessed June 19, 2023. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-covid-19
- 2020-2021 flu season summary. CDC. Updated October 25, 2021. Accessed June 19, 2023. https://www.cdc.gov/flu/season/faq-flu-season-2020-2021.htm#:~:text=What%20was%20the%202020%2D2021%20flu%20season%20like%3F
- 2021-2022 flu season summary. CDC. Updated January 12, 2023. Accessed June 19, 2023. https://www.cdc.gov/flu/season/faq-flu-season-2021-2022.htm
- Weekly U.S. influenza surveillance report. CDC. Updated June 16, 2023. Accessed June 19, 2023. https://www.cdc.gov/flu/weekly/index.htm#ILIMap
- FluView summary ending on October 1, 2022. CDC. Updated October 7, 2022. Accessed June 19, 2023. https://www.cdc.gov/flu/weekly/weeklyarchives2021-2022/week39.htm
- National, regional, and state level outpatient illness and viral surveillance, 2022-2023. FluView Interactive. Accessed June 19, 2023. https://gis.cdc.gov/grasp/fluview/fluportaldashboard.html
- Types of influenza viruses. CDC. March 30, 2023. Accessed June 19, 2023. https://www.cdc.gov/flu/about/viruses/types.htm
- Past pandemics. CDC. August 10, 2018. Accessed May 23, 2022. https://www.cdc.gov/flu/pandemic-resources/basics/past-pandemics.html
- Selecting viruses for the seasonal influenza vaccine. CDC. November 3, 2022. Accessed June 19, 2023. https://www.cdc.gov/flu/prevent/vaccineselection.htm
- How flu viruses can change: "drift" and "shift." CDC. December 12, 2022. Accessed June 19, 2022. https://www.cdc.gov/flu/about/viruses/change.htm
- How influenza (flu) vaccines are made. CDC. November 3, 2022. Accessed June 19, 2023. https://www.cdc.gov/flu/prevent/how-fluvaccine-made.htm
- Cell-based flu vaccines. CDC. September 2, 2022. Accessed June 19, 2023. https://www.cdc.gov/flu/prevent/cell-based.htm
- Recombinant influenza (flu) vaccine. CDC. August 25, 2022. Accessed June 19, 2023. https://www.cdc.gov/flu/prevent/qa_flublok-vaccine.htm
- Summary minutes. 180th Vaccines and Related Biological Products Advisory Committee. US Food and Drug Administration. March 7, 2023. Accessed June 19, 2023. https://www.fda.gov/media/166774/download
- Seasonal flu vaccines. CDC. August 25, 2022. Accessed June 19, 2023. https://www.cdc.gov/flu/prevent/flushot.htm
- McLean HQ, Petrie JG, Hanson KE, et al. Interim estimates of 2022-23 seasonal influenza vaccine effectiveness—Wisconsin, October 2022- February 2023. MMWR Morb Mortal Wkly Rep. 2023;72:201-205. doi:10.15585/mmwr.mm7208a1
- Price AM, Flannery B, Talbot HK, et al. Influenza vaccine effectiveness against influenza A(H3N2)-related illness in the United States during the 2021-2022 influenza season. Clin Infect Dis. 2023;76(8):1358-1363. doi:10.1093/cid/ciac941
- Past seasons vaccine effectiveness estimates. CDC. June 2, 2023. Accessed June 19, 2023. https://www.cdc.gov/flu/vaccines-work/past-seasonsestimates.html
- Weekly flu vaccination dashboard. CDC. Updated April 28, 2023. Accessed June 19, 2023. https://www.cdc.gov/flu/fluvaxview/dashboard/vaccination-dashboard.html
- Influenza vaccination coverage, adults. CDC. April 28, 2023. 2023. Accessed June 19, 2023. https://www.cdc.gov/flu/fluvaxview/dashboard/vaccination-adult-coverage.html
- Strategies for increasing adult vaccination rates. CDC. August 23, 2021. Accessed June 19, 2023. https://www.cdc.gov/vaccines/hcp/adults/forpractice/increasing-vacc-rates.html
- Influenza vaccination coverage, children 6 months through 17 years, United States. CDC. April 28, 2023. 2023. Accessed June 19, 2023. https://www.cdc.gov/flu/fluvaxview/dashboard/vaccination-coverage-race.html
- Protect your patients this flu season: pharmacist guide and talking points. CDC. Updated August 2022. Accessed June 19, 2023. https://www.cdc.gov/flu/pdf/professionals/vaccination/flu_hcp_pharmacisttalkingpoints_2022.pdf
Comments
Post a Comment